
Consensus for Clinicians
A practical guide for clinicians on using Consensus to find, evaluate, and apply research evidence in real-world patient care.

Dr. Benita Olivier
Professor of Rehabilitation Oxford Brookes University

01
A story worth telling
It is 1802. A patient is suffering from severe depression. She visits a physician who straps her into a whirling chair and spins her around and around until she passes out. The physician assures her this will help. It does not. She leaves traumatised and never returns.
This practice, known as rotation therapy, was used for decades. Physicians believed that spinning rearranged the disordered contents of the brain. No one asked whether it worked. No one considered whether it caused harm.
We may be tempted to shake our heads at this — but think about it: which of our current practices will be viewed with the same disbelief a hundred years from now? Evidence-based practice exists precisely to protect our patients from well-intentioned but unexamined care. And it starts, always, with asking a good question.
02
What is evidence-based practice?
The most widely used definition of evidence-based practice, also referred to as evidence-based medicine, comes from Sackett and colleagues (1996):
The evidence-based practice model has evolved considerably since Sackett’s original framework. A more comprehensive model by Satterfield et al (2009) recognises four interconnected domains:
1
best available research evidence.
2
client/population characteristics, state, needs, values, and preferences.
3
resources including clinical expertise.
4
the broader environmental and organisational context within which all of this takes place.
Why ask a better question?
Ask the right question, and you’ll find better evidence. Consensus can help you find the right information — for this patient, right now.
03
The eight steps of evidence-based practice
Evidence-based practice is sometimes presented as a neat, linear checklist. In reality, it is a thinking process — iterative, reflexive, and responsive to what you discover along the way. The eight steps below provide a useful scaffold, but they are not a script.
Step | What you’re doing | In brief |
|---|---|---|
01 | Assess your patient | Conduct a thorough clinical assessment and identify the specific questions your patient’s needs are raising. |
02 | Formulate the clinical question | Use a structured framework (PICO, SPIDER, PEO) to turn the clinical need into a searchable, neutral question. |
03 | Locate the relevant research | Search for the best available evidence using appropriate tools and databases. |
04 | Critically appraise the evidence | Evaluate the quality, relevance, and applicability of what you’ve found. Not all research is equal. |
05 | Discuss options with your patient | Bring the evidence into conversation with your patient’s values, goals, circumstances, and preferences. |
06 | Formulate the intervention plan | Draw together the research, clinical expertise, and patient context to build a tailored plan. |
07 | Implement the intervention plan | Put the plan into practice with appropriate documentation and adaptation as needed. |
08 | Evaluate and reflect | Assess whether the intervention achieved what you intended — and feed that learning back into your practice. |
These steps are sometimes summarised as the five A’s: Ask, Acquire, Appraise, Apply, Assess — a useful shorthand for clinical settings (Dawes et al., 2005), though the full eight-step model offers greater depth for complex decision-making.
04
What is Consensus — and where does it fit?
Consensus is an AI-powered research tool that searches over 200 million peer-reviewed academic papers and returns real, citable findings — with no fabricated references, no invented citations, and no confident-sounding guesswork.
Unlike a general-purpose AI chatbot, Consensus does not generate text from its training data and hope for the best. It retrieves actual published studies and uses AI to synthesise what those studies say. This makes it significantly more reliable for clinical evidence discovery than tools such as ChatGPT or Claude when used without verification.
Consensus sits most naturally within Step 3 of the EBP model — locating the relevant research. It can also support Step 4 by helping you understand a paper once you’ve found it.
Know the limit
Consensus can show you what the research says. It cannot tell you what it means for your patient. That judgement — shaped by your clinical expertise, your patient’s circumstances, and the full weight of the evidence-based model — is yours.
05
Using Consensus step by step — a worked example
Let’s walk through the EBP process with a real clinical question. Your patient is a 52-year-old with chronic lower back pain. They’ve heard that exercise might help and are asking whether it’s worth trying.
STEP 1
Assess your patient
Before you search for anything, assess thoroughly. What is the nature and duration of the pain? What has already been tried? What are your patient’s goals — return to work, improved sleep, reduced reliance on analgesia? A good clinical assessment generates the raw material for a good question.
STEP 2
Formulate the clinical question
Use the PICO framework to build a structured, neutral question. Avoid language that assumes an outcome — “Does exercise relieve back pain?” tilts your search towards positive findings before you’ve reviewed a single paper.
Worked example: PICO
P
Patient/population:
adult patients with chronic lower back pain
I
Intervention:
structured exercise programme
C
Comparison:
no structured exercise / usual care
O
Outcome:
pain levels, quality of life
Question:
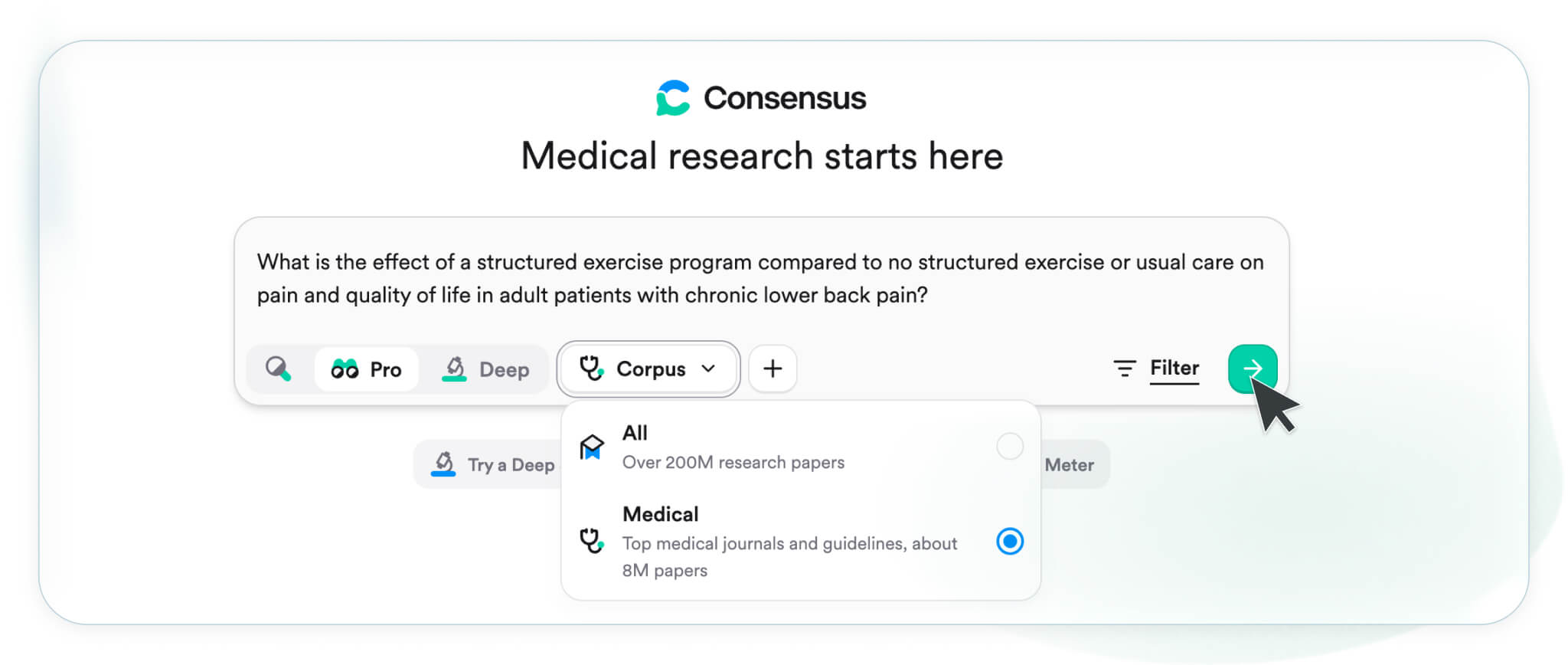
What is the effect of a structured exercise programme compared to no structured exercise or usual care on pain and quality of life in adult patients with chronic lower back pain?
Note how the question is specific, neutral, and answerable. Cross-reference with Prompting for Consensus for the full range of frameworks and Ask it right for guidance on avoiding leading language.
Consensus tip:
Consensus searches across 200M+ papers, but in clinical contexts, more isn’t always better. Medical Mode narrows your search to ~8M high-quality sources, including clinical guidelines and top-tier journals like NEJM, JAMA, and Cochrane Reviews.
Use it when you need:
- Guideline-backed answers
- Map your research themes
- Identify key databases
- Start building your systematic approach to literature review excellence
Activate it via the source dropdown in the search bar. Think of it as raising the baseline quality of the evidence you’re reviewing — not replacing your clinical judgement.
STEP 3
Search Consensus
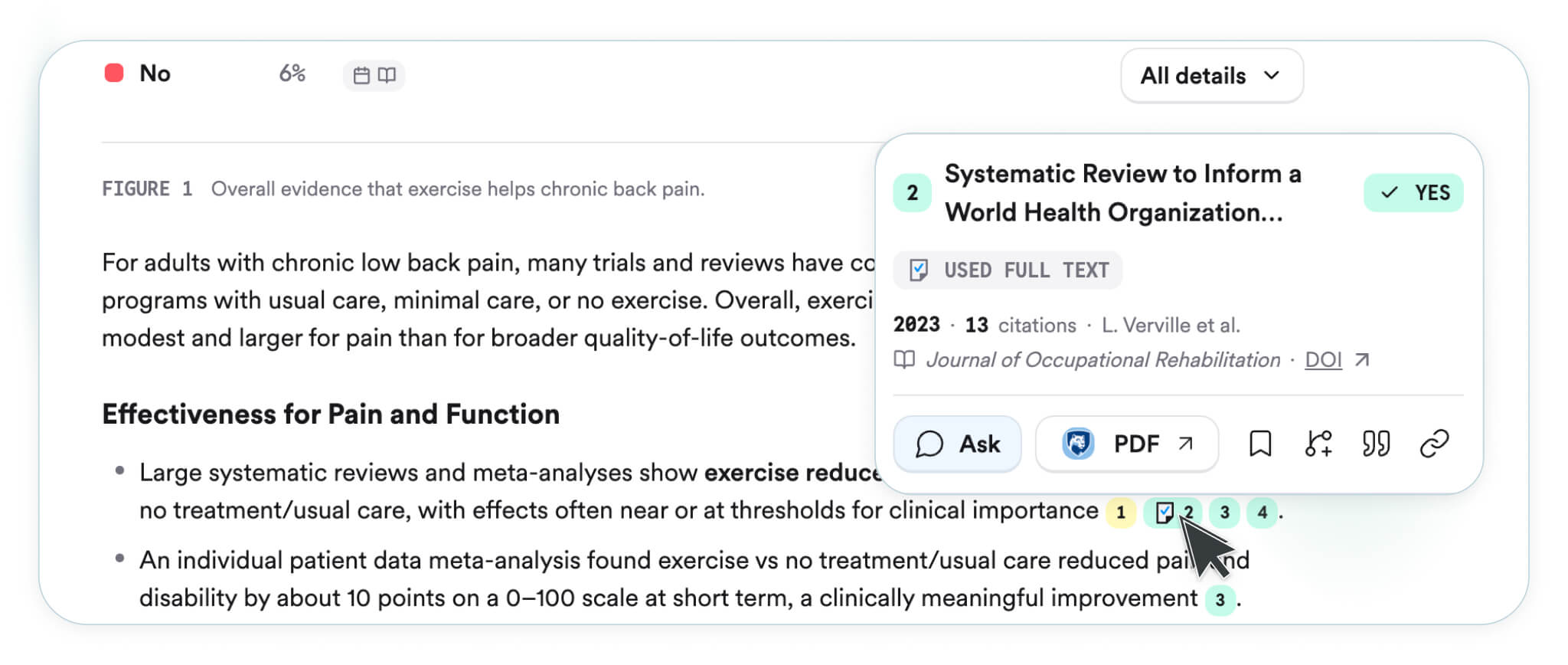
Paste your PICO question directly into Consensus. You will receive a Consensus Meter if there is enough evidence — a visual indication of whether the evidence tends to support, oppose, or remain inconclusive on the question. Read this as a starting point, not a verdict.
Scan the AI summary, then move immediately to the individual papers. Start with the highest level of evidence available: systematic reviews and clinical practice guidelines first, then randomised controlled trials, then other study designs. Consensus surfaces these for you — your job is to prioritise wisely and read critically.
A note on workflow
The AI summary in Consensus is an orientation tool. It tells you what the literature broadly says. It does not replace reading the studies. Begin with the summary to get your bearings — then go to the papers.
STEP 4
Critically appraise what you find
Finding a paper is not the same as knowing what to do with it. Not all research is equally trustworthy, and not all trustworthy research applies to your patient. When appraising what Consensus returns, ask:
What type of study is this — and where does it sit in the hierarchy of evidence?
Was the study population similar to my patient in age, diagnosis, and clinical setting?
Are the outcome measures relevant to what matters to my patient?
Are the findings clinically meaningful?
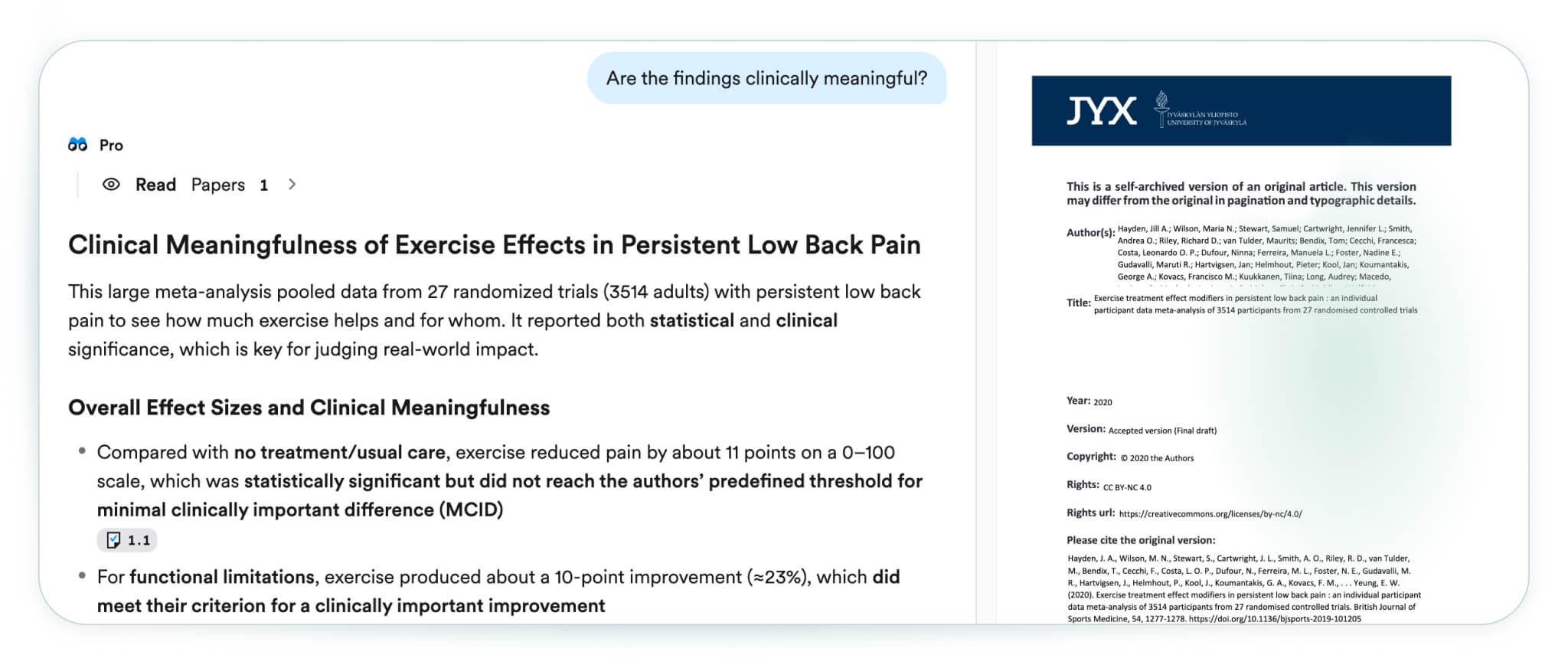
Consensus can also help you understand a paper that you’ve found. If the methodology is unfamiliar or the findings are unclear, you can ask Consensus questions directly about the study to help you clarify what you’re reading. This can be especially useful when you encounter a study design you are less familiar with. What Consensus cannot do is make the appraisal judgement on your behalf — that requires your expertise.
For a reliable, freely accessible reference on study design and levels of evidence, the Oxford Centre for Evidence-Based Medicine website offers a comprehensive hierarchy widely used in clinical practice.
STEP 5
Discuss options with your patient
The evidence cannot be applied in isolation. Bring your findings into an open conversation with your patient. In our lower back pain example, the evidence may support exercise broadly, but does your patient have the motivation, capacity, and access to follow a structured programme? What does exercise mean to them? What has put them off before?
STEPS 6, 7 AND 8
Plan, implement, and reflect
Draw together the research evidence, your clinical expertise, and your patient’s context to formulate an individualised intervention plan. Document your reasoning. Implement with appropriate monitoring and be willing to adapt.
Then evaluate:
Did it work?
What did the patient experience?
What would you do differently?
The evidence-based practice cycle does not end at implementation. Reflection feeds the next clinical question — and makes you a better clinician in the process.
06
What Consensus can and cannot do
Consensus is a powerful tool for clinical evidence discovery. Used well, it can save hours and surface research you might not have found otherwise. But it has real limits — and knowing them is part of using it responsibly.
Consensus can help you… | Consensus cannot… |
|---|---|
Find real, citable papers quickly across a large database | Replace structured database searching on MEDLINE or CINAHL, for example, for systematic reviews |
Summarise findings across multiple studies to orient your reading | Appraise the quality or methodological rigour of a study |
Identify relevant research across disciplines and specialities | Tell you whether the findings apply to your specific patient’s context |
Ask questions about a paper to clarify its methods or findings | Make the clinical decision — or take professional responsibility for it |
Generate useful search terms to take to clinical databases | Correct for bias in the published literature or gaps in what was never published |
Your pre- and post-search Checklist
Before you search:
I have assessed my patient and identified a specific clinical need.
I have a neutral, well-framed clinical question using an appropriate framework (PICO, SPIDER, PEO).
My question does not assume a direction of effect — I am asking what the evidence says, not confirming what I expect.
After you search:
I have read the original papers, not just the AI summaries.
I have considered the hierarchy of evidence and prioritised accordingly.
I have used Consensus to ask questions about individual studies to help clarify anything that was unclear in a paper.
I have considered whether the populations studied match my patient’s context.
I have noted where evidence is absent or inconclusive — absence of evidence is itself a finding.
I have disclosed my use of Consensus in line with my institution’s guidance.
Pause and reflect:
After your next Consensus search, set the output aside and write — without referring to it — one paragraph summarising what the evidence says and what it means for your patient. If you can do it fluently, you were cognitively present. If you struggle, that’s useful information: go back to the papers before you move on.
A final thought
Consensus is a remarkable tool for finding that evidence. But the clinician who knows how to ask the right question, read a paper critically, and make a sound decision in the context of a real patient — that is irreplaceable.
You are the clinician. Consensus is the tool. Use it well.
References
Dawes, M., Summerskill, W., Glasziou, P., Cartabellotta, A., Martin, J., Hopayian, K., Porzsolt, F., Burls, A., & Osborne, J. (2005). Sicily statement on evidence-based practice. BMC Medical Education, 5(1), 1.
Sackett, D.L., Rosenberg, W.M.C., Gray, J.A.M., Haynes, R.B., & Richardson, W.S. (1996). Evidence based medicine: what it is and what it isn’t. BMJ, 312(7023), 71–72.
Satterfield, J.M., Spring, B., Brownson, R.C., Mullen, E.J., Newhouse, R.P., Walker, B.B., & Whitlock, E.P. (2009). Toward a transdisciplinary model of evidence-based practice. Milbank Quarterly, 87(2), 368–390.
01
A story worth telling
It is 1802. A patient is suffering from severe depression. She visits a physician who straps her into a whirling chair and spins her around and around until she passes out. The physician assures her this will help. It does not. She leaves traumatised and never returns.
This practice, known as rotation therapy, was used for decades. Physicians believed that spinning rearranged the disordered contents of the brain. No one asked whether it worked. No one considered whether it caused harm.
We may be tempted to shake our heads at this — but think about it: which of our current practices will be viewed with the same disbelief a hundred years from now? Evidence-based practice exists precisely to protect our patients from well-intentioned but unexamined care. And it starts, always, with asking a good question.
02
What is evidence-based practice?
The most widely used definition of evidence-based practice, also referred to as evidence-based medicine, comes from Sackett and colleagues (1996):
The evidence-based practice model has evolved considerably since Sackett’s original framework. A more comprehensive model by Satterfield et al (2009) recognises four interconnected domains:
1
best available research evidence.
2
client/population characteristics, state, needs, values, and preferences.
3
resources including clinical expertise.
4
the broader environmental and organisational context within which all of this takes place.
Why ask a better question?
Ask the right question, and you’ll find better evidence. Consensus can help you find the right information — for this patient, right now.
03
The eight steps of evidence-based practice
Evidence-based practice is sometimes presented as a neat, linear checklist. In reality, it is a thinking process — iterative, reflexive, and responsive to what you discover along the way. The eight steps below provide a useful scaffold, but they are not a script.
Step | What you’re doing | In brief |
|---|---|---|
01 | Assess your patient | Conduct a thorough clinical assessment and identify the specific questions your patient’s needs are raising. |
02 | Formulate the clinical question | Use a structured framework (PICO, SPIDER, PEO) to turn the clinical need into a searchable, neutral question. |
03 | Locate the relevant research | Search for the best available evidence using appropriate tools and databases. |
04 | Critically appraise the evidence | Evaluate the quality, relevance, and applicability of what you’ve found. Not all research is equal. |
05 | Discuss options with your patient | Bring the evidence into conversation with your patient’s values, goals, circumstances, and preferences. |
06 | Formulate the intervention plan | Draw together the research, clinical expertise, and patient context to build a tailored plan. |
07 | Implement the intervention plan | Put the plan into practice with appropriate documentation and adaptation as needed. |
08 | Evaluate and reflect | Assess whether the intervention achieved what you intended — and feed that learning back into your practice. |
These steps are sometimes summarised as the five A’s: Ask, Acquire, Appraise, Apply, Assess — a useful shorthand for clinical settings (Dawes et al., 2005), though the full eight-step model offers greater depth for complex decision-making.
04
What is Consensus — and where does it fit?
Consensus is an AI-powered research tool that searches over 200 million peer-reviewed academic papers and returns real, citable findings — with no fabricated references, no invented citations, and no confident-sounding guesswork.
Unlike a general-purpose AI chatbot, Consensus does not generate text from its training data and hope for the best. It retrieves actual published studies and uses AI to synthesise what those studies say. This makes it significantly more reliable for clinical evidence discovery than tools such as ChatGPT or Claude when used without verification.
Consensus sits most naturally within Step 3 of the EBP model — locating the relevant research. It can also support Step 4 by helping you understand a paper once you’ve found it.
Know the limit
Consensus can show you what the research says. It cannot tell you what it means for your patient. That judgement — shaped by your clinical expertise, your patient’s circumstances, and the full weight of the evidence-based model — is yours.
05
Using Consensus step by step — a worked example
Let’s walk through the EBP process with a real clinical question. Your patient is a 52-year-old with chronic lower back pain. They’ve heard that exercise might help and are asking whether it’s worth trying.
STEP 1
Assess your patient
Before you search for anything, assess thoroughly. What is the nature and duration of the pain? What has already been tried? What are your patient’s goals — return to work, improved sleep, reduced reliance on analgesia? A good clinical assessment generates the raw material for a good question.
STEP 2
Formulate the clinical question
Use the PICO framework to build a structured, neutral question. Avoid language that assumes an outcome — “Does exercise relieve back pain?” tilts your search towards positive findings before you’ve reviewed a single paper.
Worked example: PICO
P
Patient/population:
adult patients with chronic lower back pain
I
Intervention:
structured exercise programme
C
Comparison:
no structured exercise / usual care
O
Outcome:
pain levels, quality of life
Question:
What is the effect of a structured exercise programme compared to no structured exercise or usual care on pain and quality of life in adult patients with chronic lower back pain?
Note how the question is specific, neutral, and answerable. Cross-reference with Prompting for Consensus for the full range of frameworks and Ask it right for guidance on avoiding leading language.
Consensus tip:
Consensus searches across 200M+ papers, but in clinical contexts, more isn’t always better. Medical Mode narrows your search to ~8M high-quality sources, including clinical guidelines and top-tier journals like NEJM, JAMA, and Cochrane Reviews.
Use it when you need:
- Guideline-backed answers
- Map your research themes
- Identify key databases
- Start building your systematic approach to literature review excellence
Activate it via the source dropdown in the search bar. Think of it as raising the baseline quality of the evidence you’re reviewing — not replacing your clinical judgement.
STEP 3
Search Consensus
Paste your PICO question directly into Consensus. You will receive a Consensus Meter if there is enough evidence — a visual indication of whether the evidence tends to support, oppose, or remain inconclusive on the question. Read this as a starting point, not a verdict.
Scan the AI summary, then move immediately to the individual papers. Start with the highest level of evidence available: systematic reviews and clinical practice guidelines first, then randomised controlled trials, then other study designs. Consensus surfaces these for you — your job is to prioritise wisely and read critically.
A note on workflow
The AI summary in Consensus is an orientation tool. It tells you what the literature broadly says. It does not replace reading the studies. Begin with the summary to get your bearings — then go to the papers.
STEP 4
Critically appraise what you find
Finding a paper is not the same as knowing what to do with it. Not all research is equally trustworthy, and not all trustworthy research applies to your patient. When appraising what Consensus returns, ask:
What type of study is this — and where does it sit in the hierarchy of evidence?
Was the study population similar to my patient in age, diagnosis, and clinical setting?
Are the outcome measures relevant to what matters to my patient?
Are the findings clinically meaningful?
Consensus can also help you understand a paper that you’ve found. If the methodology is unfamiliar or the findings are unclear, you can ask Consensus questions directly about the study to help you clarify what you’re reading. This can be especially useful when you encounter a study design you are less familiar with. What Consensus cannot do is make the appraisal judgement on your behalf — that requires your expertise.
For a reliable, freely accessible reference on study design and levels of evidence, the Oxford Centre for Evidence-Based Medicine website offers a comprehensive hierarchy widely used in clinical practice.
STEP 5
Discuss options with your patient
The evidence cannot be applied in isolation. Bring your findings into an open conversation with your patient. In our lower back pain example, the evidence may support exercise broadly, but does your patient have the motivation, capacity, and access to follow a structured programme? What does exercise mean to them? What has put them off before?
STEPS 6, 7 AND 8
Plan, implement, and reflect
Draw together the research evidence, your clinical expertise, and your patient’s context to formulate an individualised intervention plan. Document your reasoning. Implement with appropriate monitoring and be willing to adapt.
Then evaluate:
Did it work?
What did the patient experience?
What would you do differently?
The evidence-based practice cycle does not end at implementation. Reflection feeds the next clinical question — and makes you a better clinician in the process.
06
What Consensus can and cannot do
Consensus is a powerful tool for clinical evidence discovery. Used well, it can save hours and surface research you might not have found otherwise. But it has real limits — and knowing them is part of using it responsibly.
Consensus can help you… | Consensus cannot… |
|---|---|
Find real, citable papers quickly across a large database | Replace structured database searching on MEDLINE or CINAHL, for example, for systematic reviews |
Summarise findings across multiple studies to orient your reading | Appraise the quality or methodological rigour of a study |
Identify relevant research across disciplines and specialities | Tell you whether the findings apply to your specific patient’s context |
Ask questions about a paper to clarify its methods or findings | Make the clinical decision — or take professional responsibility for it |
Generate useful search terms to take to clinical databases | Correct for bias in the published literature or gaps in what was never published |
Your pre- and post-search Checklist
Before you search:
I have assessed my patient and identified a specific clinical need.
I have a neutral, well-framed clinical question using an appropriate framework (PICO, SPIDER, PEO).
My question does not assume a direction of effect — I am asking what the evidence says, not confirming what I expect.
After you search:
I have read the original papers, not just the AI summaries.
I have considered the hierarchy of evidence and prioritised accordingly.
I have used Consensus to ask questions about individual studies to help clarify anything that was unclear in a paper.
I have considered whether the populations studied match my patient’s context.
I have noted where evidence is absent or inconclusive — absence of evidence is itself a finding.
I have disclosed my use of Consensus in line with my institution’s guidance.
Pause and reflect:
After your next Consensus search, set the output aside and write — without referring to it — one paragraph summarising what the evidence says and what it means for your patient. If you can do it fluently, you were cognitively present. If you struggle, that’s useful information: go back to the papers before you move on.
A final thought
Consensus is a remarkable tool for finding that evidence. But the clinician who knows how to ask the right question, read a paper critically, and make a sound decision in the context of a real patient — that is irreplaceable.
You are the clinician. Consensus is the tool. Use it well.
References
Dawes, M., Summerskill, W., Glasziou, P., Cartabellotta, A., Martin, J., Hopayian, K., Porzsolt, F., Burls, A., & Osborne, J. (2005). Sicily statement on evidence-based practice. BMC Medical Education, 5(1), 1.
Sackett, D.L., Rosenberg, W.M.C., Gray, J.A.M., Haynes, R.B., & Richardson, W.S. (1996). Evidence based medicine: what it is and what it isn’t. BMJ, 312(7023), 71–72.
Satterfield, J.M., Spring, B., Brownson, R.C., Mullen, E.J., Newhouse, R.P., Walker, B.B., & Whitlock, E.P. (2009). Toward a transdisciplinary model of evidence-based practice. Milbank Quarterly, 87(2), 368–390.
01
A story worth telling
It is 1802. A patient is suffering from severe depression. She visits a physician who straps her into a whirling chair and spins her around and around until she passes out. The physician assures her this will help. It does not. She leaves traumatised and never returns.
This practice, known as rotation therapy, was used for decades. Physicians believed that spinning rearranged the disordered contents of the brain. No one asked whether it worked. No one considered whether it caused harm.
We may be tempted to shake our heads at this — but think about it: which of our current practices will be viewed with the same disbelief a hundred years from now? Evidence-based practice exists precisely to protect our patients from well-intentioned but unexamined care. And it starts, always, with asking a good question.
02
What is evidence-based practice?
The most widely used definition of evidence-based practice, also referred to as evidence-based medicine, comes from Sackett and colleagues (1996):
The evidence-based practice model has evolved considerably since Sackett’s original framework. A more comprehensive model by Satterfield et al (2009) recognises four interconnected domains:
1
best available research evidence.
2
client/population characteristics, state, needs, values, and preferences.
3
resources including clinical expertise.
4
the broader environmental and organisational context within which all of this takes place.
Why ask a better question?
Ask the right question, and you’ll find better evidence. Consensus can help you find the right information — for this patient, right now.
03
The eight steps of evidence-based practice
Evidence-based practice is sometimes presented as a neat, linear checklist. In reality, it is a thinking process — iterative, reflexive, and responsive to what you discover along the way. The eight steps below provide a useful scaffold, but they are not a script.
Step | What you’re doing | In brief |
|---|---|---|
01 | Assess your patient | Conduct a thorough clinical assessment and identify the specific questions your patient’s needs are raising. |
02 | Formulate the clinical question | Use a structured framework (PICO, SPIDER, PEO) to turn the clinical need into a searchable, neutral question. |
03 | Locate the relevant research | Search for the best available evidence using appropriate tools and databases. |
04 | Critically appraise the evidence | Evaluate the quality, relevance, and applicability of what you’ve found. Not all research is equal. |
05 | Discuss options with your patient | Bring the evidence into conversation with your patient’s values, goals, circumstances, and preferences. |
06 | Formulate the intervention plan | Draw together the research, clinical expertise, and patient context to build a tailored plan. |
07 | Implement the intervention plan | Put the plan into practice with appropriate documentation and adaptation as needed. |
08 | Evaluate and reflect | Assess whether the intervention achieved what you intended — and feed that learning back into your practice. |
These steps are sometimes summarised as the five A’s: Ask, Acquire, Appraise, Apply, Assess — a useful shorthand for clinical settings (Dawes et al., 2005), though the full eight-step model offers greater depth for complex decision-making.
04
What is Consensus — and where does it fit?
Consensus is an AI-powered research tool that searches over 200 million peer-reviewed academic papers and returns real, citable findings — with no fabricated references, no invented citations, and no confident-sounding guesswork.
Unlike a general-purpose AI chatbot, Consensus does not generate text from its training data and hope for the best. It retrieves actual published studies and uses AI to synthesise what those studies say. This makes it significantly more reliable for clinical evidence discovery than tools such as ChatGPT or Claude when used without verification.
Consensus sits most naturally within Step 3 of the EBP model — locating the relevant research. It can also support Step 4 by helping you understand a paper once you’ve found it.
Know the limit
Consensus can show you what the research says. It cannot tell you what it means for your patient. That judgement — shaped by your clinical expertise, your patient’s circumstances, and the full weight of the evidence-based model — is yours.
05
Using Consensus step by step — a worked example
Let’s walk through the EBP process with a real clinical question. Your patient is a 52-year-old with chronic lower back pain. They’ve heard that exercise might help and are asking whether it’s worth trying.
STEP 1
Assess your patient
Before you search for anything, assess thoroughly. What is the nature and duration of the pain? What has already been tried? What are your patient’s goals — return to work, improved sleep, reduced reliance on analgesia? A good clinical assessment generates the raw material for a good question.
STEP 2
Formulate the clinical question
Use the PICO framework to build a structured, neutral question. Avoid language that assumes an outcome — “Does exercise relieve back pain?” tilts your search towards positive findings before you’ve reviewed a single paper.
Worked example: PICO
P
Patient/population:
adult patients with chronic lower back pain
I
Intervention:
structured exercise programme
C
Comparison:
no structured exercise / usual care
O
Outcome:
pain levels, quality of life
Question:
What is the effect of a structured exercise programme compared to no structured exercise or usual care on pain and quality of life in adult patients with chronic lower back pain?
Note how the question is specific, neutral, and answerable. Cross-reference with Prompting for Consensus for the full range of frameworks and Ask it right for guidance on avoiding leading language.
Consensus tip:
Consensus searches across 200M+ papers, but in clinical contexts, more isn’t always better. Medical Mode narrows your search to ~8M high-quality sources, including clinical guidelines and top-tier journals like NEJM, JAMA, and Cochrane Reviews.
Use it when you need:
- Guideline-backed answers
- Map your research themes
- Identify key databases
- Start building your systematic approach to literature review excellence
Activate it via the source dropdown in the search bar. Think of it as raising the baseline quality of the evidence you’re reviewing — not replacing your clinical judgement.
STEP 3
Search Consensus
Paste your PICO question directly into Consensus. You will receive a Consensus Meter if there is enough evidence — a visual indication of whether the evidence tends to support, oppose, or remain inconclusive on the question. Read this as a starting point, not a verdict.
Scan the AI summary, then move immediately to the individual papers. Start with the highest level of evidence available: systematic reviews and clinical practice guidelines first, then randomised controlled trials, then other study designs. Consensus surfaces these for you — your job is to prioritise wisely and read critically.
A note on workflow
The AI summary in Consensus is an orientation tool. It tells you what the literature broadly says. It does not replace reading the studies. Begin with the summary to get your bearings — then go to the papers.
STEP 4
Critically appraise what you find
Finding a paper is not the same as knowing what to do with it. Not all research is equally trustworthy, and not all trustworthy research applies to your patient. When appraising what Consensus returns, ask:
What type of study is this — and where does it sit in the hierarchy of evidence?
Was the study population similar to my patient in age, diagnosis, and clinical setting?
Are the outcome measures relevant to what matters to my patient?
Are the findings clinically meaningful?
Consensus can also help you understand a paper that you’ve found. If the methodology is unfamiliar or the findings are unclear, you can ask Consensus questions directly about the study to help you clarify what you’re reading. This can be especially useful when you encounter a study design you are less familiar with. What Consensus cannot do is make the appraisal judgement on your behalf — that requires your expertise.
For a reliable, freely accessible reference on study design and levels of evidence, the Oxford Centre for Evidence-Based Medicine website offers a comprehensive hierarchy widely used in clinical practice.
STEP 5
Discuss options with your patient
The evidence cannot be applied in isolation. Bring your findings into an open conversation with your patient. In our lower back pain example, the evidence may support exercise broadly, but does your patient have the motivation, capacity, and access to follow a structured programme? What does exercise mean to them? What has put them off before?
STEPS 6, 7 AND 8
Plan, implement, and reflect
Draw together the research evidence, your clinical expertise, and your patient’s context to formulate an individualised intervention plan. Document your reasoning. Implement with appropriate monitoring and be willing to adapt.
Then evaluate:
Did it work?
What did the patient experience?
What would you do differently?
The evidence-based practice cycle does not end at implementation. Reflection feeds the next clinical question — and makes you a better clinician in the process.
06
What Consensus can and cannot do
Consensus is a powerful tool for clinical evidence discovery. Used well, it can save hours and surface research you might not have found otherwise. But it has real limits — and knowing them is part of using it responsibly.
Consensus can help you… | Consensus cannot… |
|---|---|
Find real, citable papers quickly across a large database | Replace structured database searching on MEDLINE or CINAHL, for example, for systematic reviews |
Summarise findings across multiple studies to orient your reading | Appraise the quality or methodological rigour of a study |
Identify relevant research across disciplines and specialities | Tell you whether the findings apply to your specific patient’s context |
Ask questions about a paper to clarify its methods or findings | Make the clinical decision — or take professional responsibility for it |
Generate useful search terms to take to clinical databases | Correct for bias in the published literature or gaps in what was never published |
Your pre- and post-search Checklist
Before you search:
I have assessed my patient and identified a specific clinical need.
I have a neutral, well-framed clinical question using an appropriate framework (PICO, SPIDER, PEO).
My question does not assume a direction of effect — I am asking what the evidence says, not confirming what I expect.
After you search:
I have read the original papers, not just the AI summaries.
I have considered the hierarchy of evidence and prioritised accordingly.
I have used Consensus to ask questions about individual studies to help clarify anything that was unclear in a paper.
I have considered whether the populations studied match my patient’s context.
I have noted where evidence is absent or inconclusive — absence of evidence is itself a finding.
I have disclosed my use of Consensus in line with my institution’s guidance.
Pause and reflect:
After your next Consensus search, set the output aside and write — without referring to it — one paragraph summarising what the evidence says and what it means for your patient. If you can do it fluently, you were cognitively present. If you struggle, that’s useful information: go back to the papers before you move on.
A final thought
Consensus is a remarkable tool for finding that evidence. But the clinician who knows how to ask the right question, read a paper critically, and make a sound decision in the context of a real patient — that is irreplaceable.
You are the clinician. Consensus is the tool. Use it well.
References
Dawes, M., Summerskill, W., Glasziou, P., Cartabellotta, A., Martin, J., Hopayian, K., Porzsolt, F., Burls, A., & Osborne, J. (2005). Sicily statement on evidence-based practice. BMC Medical Education, 5(1), 1.
Sackett, D.L., Rosenberg, W.M.C., Gray, J.A.M., Haynes, R.B., & Richardson, W.S. (1996). Evidence based medicine: what it is and what it isn’t. BMJ, 312(7023), 71–72.
Satterfield, J.M., Spring, B., Brownson, R.C., Mullen, E.J., Newhouse, R.P., Walker, B.B., & Whitlock, E.P. (2009). Toward a transdisciplinary model of evidence-based practice. Milbank Quarterly, 87(2), 368–390.
Become a Consensus MCP expert.
For courses and more information on how to use the MCP, check out our guide below.

Empowering the world to accelerate research.
Empowering the world to accelerate research.
Empowering the world to accelerate research.
Example: